 English
English  Español
Español  Português
Português 
There is a group of muscles in the female body that carries enormous responsibility — supporting the bladder, bowel, and uterus, contributing to core stability, playing a role in sexual function, and bearing the full weight of pregnancy. Yet these muscles rarely make an appearance in mainstream fitness culture. They cannot be seen in a mirror. They do not show up in before-and-after photos. And for most women, they go completely unexercised until something goes wrong.
The pelvic floor is not a single muscle. It is a hammock-like group of muscles, ligaments, and connective tissues that forms the base of the pelvis. Understanding how this structure works — and what science tells us about keeping it healthy — is one of the more practical things a woman can do for her long-term physical wellbeing.
In Brief
What this article covers
- What the pelvic floor is and why it matters
- How to correctly identify and engage these muscles
- The core exercises research supports most
- How pregnancy and aging change pelvic floor health
- Common mistakes women make — and how to avoid them
What Exactly Is the Pelvic Floor?
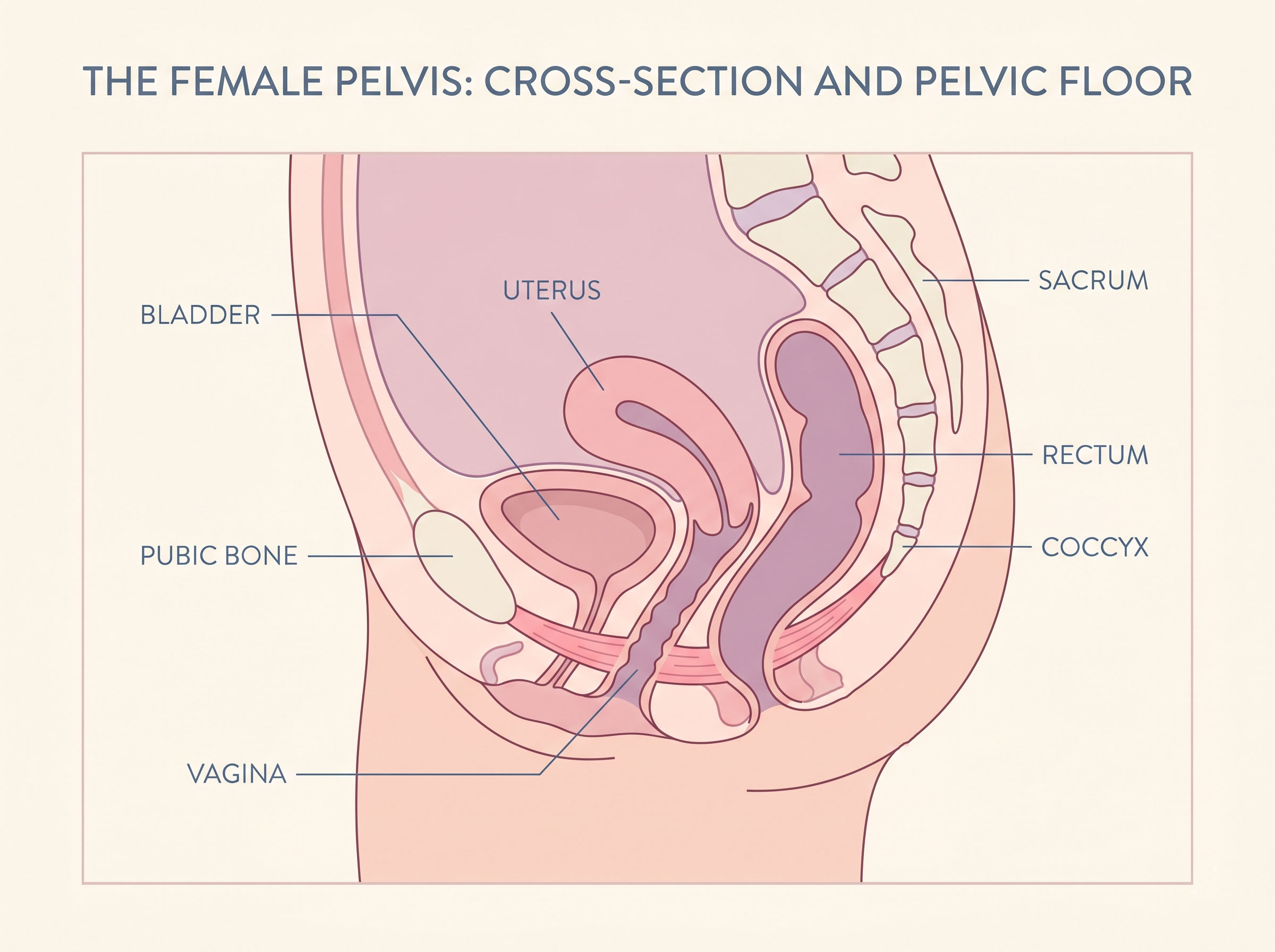
Picture the pelvis as a bowl. The pelvic floor forms the base of that bowl — a layered system of muscles stretching from the tailbone at the back to the pubic bone at the front, and from one sitting bone to the other on each side. This muscular base has three openings in women: the urethra, the vagina, and the anus.
Cultural Insight
Ancient Wisdom, Modern Validation
Traditional Chinese medicine practitioners and certain Daoist health traditions have referenced the pelvic region as a center of vital energy for centuries. Practices like qi gong included deliberate engagement of the pelvic floor as part of cultivating internal strength — long before the term "Kegel" existed in any language.
In India, classical texts on women's postpartum recovery described exercises that modern physiotherapists recognize as early descriptions of pelvic floor retraining — tradition and science arriving at the same place by different roads.
These muscles work continuously and largely without conscious thought. They contract to keep the bladder and bowel closed, relax to allow urination or bowel movements, support the uterus during pregnancy, and work in coordination with the deep abdominal muscles, the diaphragm, and the muscles along the spine to stabilize the entire trunk.
Research has shown that pelvic floor dysfunction — which includes symptoms such as urinary leakage, pelvic organ prolapse, pelvic pain, and difficulties with bowel function — is remarkably common among women. Studies published in journals including the American Journal of Obstetrics and Gynecology have estimated that roughly one in three women will experience some form of pelvic floor disorder in her lifetime. Childbirth, aging, hormonal changes, and certain types of high-impact exercise are all factors that influence pelvic floor health.
The good news is that pelvic floor muscles respond to training in much the same way other skeletal muscles do. They can be strengthened when weak, and they can be consciously relaxed and lengthened when chronically tight.
Finding the Right Muscles First
One of the most consistent findings in pelvic floor research is that a significant proportion of women — some studies suggest as many as 30 percent — perform pelvic floor exercises incorrectly when not guided by a professional. The most common error is bearing down (pushing outward and downward) rather than lifting inward and upward. Doing so over time may actually worsen pelvic floor symptoms rather than improve them.
"A significant proportion of women perform pelvic floor exercises incorrectly when not guided by a professional — the most common error is pushing out rather than lifting in."
Research FindingBefore beginning any pelvic floor exercise program, the first task is accurate muscle identification. Here are several reliable techniques that women and physiotherapists commonly use:
The stop-flow test (for identification only, not exercise): While urinating, try briefly pausing the flow of urine. The muscles you use to do this are part of the pelvic floor. This technique should be used only once or twice to learn which muscles to engage — not repeated as a regular exercise, as doing so may interfere with normal bladder function.
Internal awareness: Sitting or lying comfortably, imagine picking up a small marble using only the muscles at the vaginal opening. That sensation of inward lift — not of tightening the buttocks or inner thighs — is the target engagement.
Breathing into the pelvis: Take a slow, full breath in, allowing the lower belly to rise and the pelvic floor to naturally lower and soften. On the exhale, gently draw the pelvic floor upward. This breath-coordinated approach is widely used in women's health physiotherapy and helps build body awareness before adding any strength component.
The Exercises That Research Supports
The following exercises are drawn from established women's health physiotherapy practice and the scientific literature on pelvic floor rehabilitation. They are appropriate for most healthy women as a starting point — women recovering from recent childbirth, pelvic surgery, or experiencing active pelvic pain should seek guidance from a qualified pelvic floor physiotherapist before beginning.
Quick-Start Guide
Before You Begin: Tools & Tips
✓ DO
- Empty your bladder before exercising
- Breathe normally throughout
- Start slowly and build gradually
- Practice consistently — daily if possible
- Rest fully between contractions
✗ DON'T
- Hold your breath or brace your abdomen
- Clench your buttocks or inner thighs
- Use the stop-flow test as regular exercise
- Push outward/downward instead of lifting up
- Expect overnight results — allow weeks
1. The Standard Kegel Contraction
Named after American gynaecologist Dr. Arnold Kegel, who first published research on pelvic floor exercises in the late 1940s, the Kegel contraction remains the foundation of pelvic floor training. Research published through the Cochrane Collaboration on pelvic floor muscle training consistently shows it to be effective in reducing urinary incontinence in women.
How to perform it: In a comfortable seated or lying position, inhale to prepare. On your exhale, gently draw the pelvic floor upward — thinking of that lift through all three openings simultaneously. Hold the contraction for three to five seconds while breathing normally. Release fully and rest for an equal amount of time. Repeat eight to twelve times per set, aiming for three sets throughout the day.
As strength builds over several weeks, the goal is to progress toward holding each contraction for ten seconds, with ten repetitions per set.
2. The Quick-Flick Contraction
Where the standard Kegel trains endurance and resting tone, the quick-flick focuses on the fast-twitch muscle fibers of the pelvic floor — the fibers that respond rapidly to sudden increases in abdominal pressure such as a cough, sneeze, or jump.
Many women who experience stress urinary incontinence — the leaking that can accompany sneezing or jumping — have under-trained fast-twitch fibers. This exercise specifically targets that gap.
How to perform it: Contract the pelvic floor quickly and firmly upward, then release immediately and completely. The entire cycle — lift, release — should take about one second. Repeat ten times, then rest. This exercise can follow a set of standard Kegel contractions as a complement.
3. The Elevator Exercise
This exercise introduces gradations of contraction — training the pelvic floor to work at different levels of effort rather than just fully on or fully off. Women's health physiotherapists often use this approach with patients who have difficulty sensing partial engagement.
How to perform it: Visualize the pelvic floor as an elevator in a building with four floors. Floor one is a very light engagement — perhaps twenty percent of maximum effort. Floor two is a moderate engagement. Floor three is strong. Floor four is full effort. Slowly "rise" from floor to floor, pausing briefly at each level, then descend just as slowly. Rest fully before repeating. Aim for three to five repetitions.
Exercise Reference
Pelvic Floor Exercises at a Glance
| Exercise | Muscle Fibers | Primary Benefit | Reps / Sets |
|---|---|---|---|
| Standard Kegel | Slow-twitch | Resting tone, endurance, prolapse prevention | 8–12 reps × 3 sets/day |
| Quick-Flick | Fast-twitch | Stress incontinence, sneeze/cough leakage | 10 rapid reps × 3 sets/day |
| Elevator | Full spectrum | Body awareness, graded control | 3–5 reps × 2 sets/day |
| Functional Integration | Slow & fast-twitch | Real-life movement support, core coordination | Built into daily activity |
| Diaphragmatic Release | Relaxation focus | Hypertonic (tight) pelvic floor, pain reduction | 5–10 breath cycles × 2 sets/day |
4. Functional Integration
Isolated exercises are valuable for building awareness and baseline strength, but research on core function increasingly points to the importance of integrating pelvic floor engagement into everyday movement patterns. The pelvic floor should work automatically in coordination with the rest of the deep core system — but in women with dysfunction, this automatic coordination can become disrupted.
Practical functional exercises include:
The "knack" technique: A pre-contraction — squeezing and lifting the pelvic floor just before and during a cough, sneeze, or jump. Studies have found that women who learn the knack technique can significantly reduce leakage during activities of daily life within just a few weeks of consistent practice.
Pelvic floor bracing during lifting: Before lifting a child, groceries, or any weight, exhale and gently draw the pelvic floor upward first. This co-activation with the transverse abdominis creates a stable container around the spine and reduces downward pressure on the pelvic floor itself.
5. Diaphragmatic Breathing for a Tight Pelvic Floor
Not every pelvic floor problem comes from weakness. Research and clinical experience both suggest that a significant number of women with pelvic pain, painful intercourse, urinary urgency, or difficulty with bowel movements actually have a hypertonic (overly tight) pelvic floor — one that struggles to fully relax and lengthen rather than one that lacks strength.
For these women, adding more Kegel contractions may actually increase symptoms. The appropriate exercise is not contraction but release.
How to perform it: Lie on your back with knees bent and feet flat. Place one hand on the lower belly. Breathe in slowly and deeply through the nose, feeling the belly rise and consciously allowing the pelvic floor to soften, drop, and widen with each inhale — like a flower opening. The exhale should be slow and quiet. Repeat for five to ten breath cycles. This can also be practiced in a supported squat position, which naturally encourages pelvic floor lengthening.
The knack technique has been studied since the 1990s
Research by continence specialist Dr. Kathryn Burgio and colleagues at the University of Alabama found that women taught the pre-contraction technique reduced cough-related leakage by up to 98 percent in some cases — without surgery or medication. The research helped shift pelvic floor training from a post-surgical rehabilitation tool to a mainstream preventive practice.
Pregnancy, Postpartum, and the Pelvic Floor
Pregnancy places the pelvic floor under sustained and significant load. The growing uterus exerts increasing downward pressure across all three trimesters, hormonal changes — particularly the relaxin surge — loosen connective tissue to prepare the pelvis for birth, and vaginal delivery can stretch and sometimes injure pelvic floor muscles and nerves.
Studies consistently show that women who practice pelvic floor exercises during pregnancy experience lower rates of urinary incontinence in the third trimester and postpartum period compared with women who do not. The NHS guidance on pelvic floor exercises during pregnancy recommends that all pregnant women be instructed in these techniques — a recommendation shared by most major obstetric and physiotherapy bodies worldwide.
Many women report being told to "just do your Kegels" after birth without being given meaningful instruction. Research suggests this approach produces inconsistent results — and for women with pelvic floor tears or significant postpartum changes, unsupported exercise may be insufficient. Pelvic floor physiotherapy assessments at six to twelve weeks postpartum are increasingly considered standard care in many countries, including France, where postpartum pelvic rehabilitation has been publicly funded since 1985.
Worth Noting
In France, postpartum pelvic floor rehabilitation — la rééducation périnéale — has been publicly funded since the 1980s. New mothers are routinely referred for ten or more supervised physiotherapy sessions. Many women's health advocates and physiotherapists in North America have pointed to this model when calling for greater access to postpartum pelvic care.
How Aging Affects the Pelvic Floor
The decline in estrogen that accompanies perimenopause and menopause is directly linked to changes in pelvic floor tissue. Estrogen supports the elasticity and lubrication of vaginal tissue, the strength of ligaments, and the health of the connective tissue that supports pelvic organs. As levels drop, these tissues can become thinner and less resilient — a process known as genitourinary syndrome of menopause.
Research shows that regular pelvic floor muscle training in midlife and beyond can slow — though not entirely prevent — some of these changes, and that postmenopausal women who train consistently show better pelvic floor function than those who are sedentary. The evidence is strongest for urinary continence outcomes, with several systematic reviews confirming the benefit of ongoing pelvic floor training in older women.
Consistency matters more here than intensity. A moderate program maintained over years will produce better outcomes than an intensive short-term approach that is abandoned.
By the Numbers
1 in 3
women experience pelvic floor disorder in their lifetime
~30%
of women perform Kegel exercises incorrectly without guidance
1985
year France began publicly funding postpartum pelvic rehabilitation
12 wks
typical minimum before meaningful strength improvements are measurable
A Note on High-Impact Exercise and the Pelvic Floor
Running, jumping, heavy lifting, and high-intensity interval training are all associated with increased intra-abdominal pressure — pressure that the pelvic floor must manage from below. Research published in the British Journal of Sports Medicine found that leakage during exercise is far more common among female athletes than was previously acknowledged, with surveys of elite sportswomen reporting rates of 30 to 80 percent depending on the sport.
This does not mean high-impact exercise should be avoided. Rather, it means that pelvic floor training should be considered part of any active woman's fitness routine — not a separate, clinical concern but an integrated component of physical preparation in the same way that warming up the hamstrings before a run makes good mechanical sense.
Women returning to running or impact exercise after childbirth are typically advised — by organizations including the Pelvic, Obstetric and Gynaecological Physiotherapy association — to wait until at least three months postpartum and to pass specific load tests before resuming high-impact activity.
Try This at Home
A Simple 5-Minute Daily Routine
- 1 minute — Body scan: Sitting comfortably, take three slow, deep breaths. Notice whether the pelvic floor feels tense or relaxed.
- 2 minutes — Standard Kegels: Three sets of 8 contractions, holding for 5 seconds each, with 5 seconds of full release between each.
- 1 minute — Quick flicks: Ten rapid contract-and-release cycles. Rest 30 seconds. Repeat once.
- 1 minute — Deep release: Lie back and take 5 slow diaphragmatic breaths, consciously dropping and widening the pelvic floor on each inhale.
This sequence can be done in bed in the morning, during a lunch break, or before sleep. Consistency over time — weeks and months — is where the benefit accumulates.
When to Seek Professional Assessment
Self-directed exercise programs based on published guidelines are appropriate for many women with mild symptoms or as a general preventive practice. There are circumstances, however, in which professional assessment is the more appropriate starting point.
Many women report feeling reluctant to discuss pelvic floor symptoms with their doctor — research suggests that many wait years after symptoms begin before seeking help. Pelvic floor dysfunction is common, well understood, and highly treatable, particularly when addressed before symptoms become severe. Women's health physiotherapists and pelvic floor specialists are specifically trained in this area and can conduct assessments that confirm whether weakness, tightness, or coordination problems are present — guiding a training program that is targeted rather than generic.
Questions & Answers
Common Questions About Pelvic Floor Exercise
The pelvic floor sits at the intersection of movement science, women's health, and the basic mechanics of daily life. Research has made the case clearly: these muscles respond to training, dysfunction is common and underreported, and the window for intervention is wide — from the early postpartum weeks to decades beyond menopause. What has sometimes been treated as a niche concern for older women is, in fact, a foundation worth tending at every age.
Disclaimer: All content on this website—including articles, educational materials, and interactive calculators—is for informational, educational, and entertainment purposes only. The calculations, percentiles, and outputs generated by tools on this site are based on general statistical data and mathematical models; they do not constitute medical data, a clinical assessment, or a diagnosis.
Nothing contained on this website is a substitute for professional medical advice, diagnosis, or treatment. Always seek the guidance of a qualified healthcare professional or urologist with any questions you have regarding physical development, anatomy, or health conditions. Reliance on any information or tools provided by this website is solely at your own risk.





