 English
English  Español
Español  Português
Português 
The honest, science-backed guide every woman should read before—or after—she starts. Most women are handed a pill, a patch, or a prescription and sent on their way with a leaflet that lists side effects in six-point type. Nobody sits down and explains what is actually happening inside your body the moment synthetic hormones enter the picture.
That gap between "here's your prescription" and "here's what this means for your health" is exactly where confusion—and sometimes real distress—takes root.
Birth control is not a monolith. It is a broad category of methods that work through very different mechanisms, and each one carries a distinct hormonal fingerprint. Understanding those differences is not about being anti-contraception or pro-contraception. It is simply about knowing your own body well enough to make choices that feel right for your life, your cycle, and your long-term health.
Understanding what birth control does to your hormones is not about being for or against it. It is about knowing your own body deeply enough to advocate for yourself.
— Lexi PierceYour Natural Cycle: The Baseline
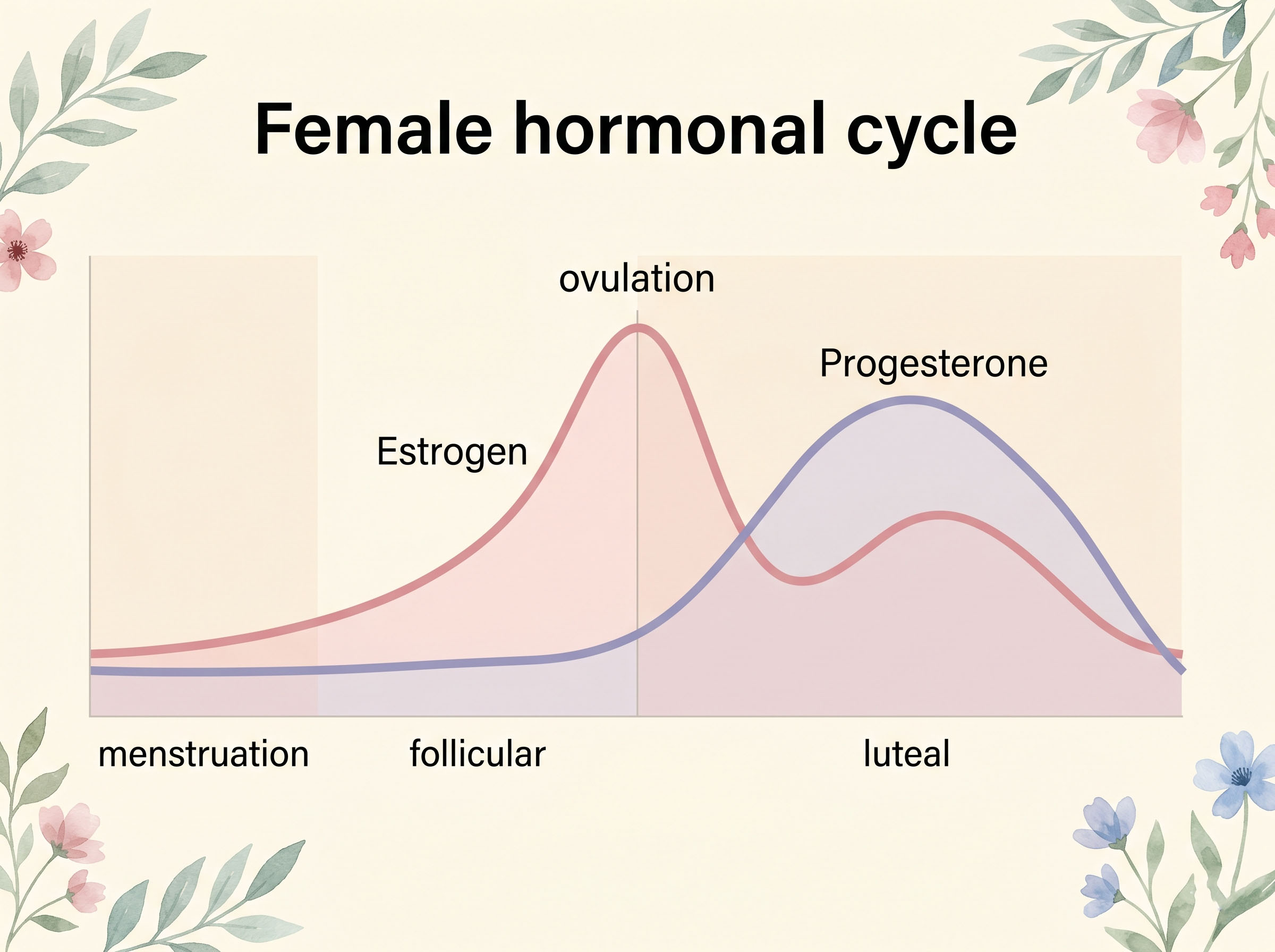
Before any conversation about synthetic hormones makes sense, it helps to understand what your body is doing on its own. A healthy menstrual cycle is not just a monthly inconvenience. It is a finely tuned hormonal symphony that influences your mood, energy, skin, libido, bone density, and even how you think.
The cycle runs on four main hormones: estrogen, progesterone, luteinizing hormone (LH), and follicle-stimulating hormone (FSH). Estrogen rises in the first half of your cycle, peaks at ovulation, and drives everything from glowing skin to social confidence. Progesterone takes over in the second half, bringing a calmer, more inward energy—sometimes tipping into PMS territory. LH and FSH are the command signals from the brain that trigger the whole process to begin.
Ovulation—the moment an egg is released—is not just about fertility. It is a monthly health event. Research from endocrinology experts, including work cited by the American College of Obstetricians and Gynecologists, confirms that ovulation itself produces the progesterone surge that protects bone density, supports thyroid function, and stabilizes mood. When a contraceptive method suppresses ovulation, that benefit disappears along with the egg.
How Combined Hormonal Methods Work
The combined oral contraceptive pill—the most widely used form of hormonal birth control—contains synthetic versions of both estrogen and progesterone, called ethinyl estradiol and a progestin. Together, they send a message to your brain's hypothalamus and pituitary gland: "Pregnancy is already underway. Stand down." The pituitary stops releasing LH and FSH, ovulation is suppressed, and your natural hormonal cycle is essentially replaced by a manufactured one.
This manufactured cycle is not identical to your natural one, even if the pill packaging calls it a "period." The bleed that happens during the pill's placebo week is a withdrawal bleed caused by the sudden drop in synthetic hormones—not an ovulatory cycle. Your body is not doing the same hormonal work it would do naturally.
The same suppression mechanism applies to the hormonal patch, the vaginal ring (NuvaRing), and the hormonal IUD, though each delivers hormones differently and in varying doses. The hormonal IUD, for example, primarily uses a progestin called levonorgestrel and works mainly locally in the uterus. Many women on the hormonal IUD continue to ovulate—though lighter periods or no periods at all are common because the uterine lining is kept thin.
By the Numbers
Birth Control Use in the United States
Sources: CDC National Center for Health Statistics; published clinical research on post-pill recovery.
The Progesterone Problem
Here is where many women's experiences start to make sense. Natural progesterone—the kind your body makes after ovulation—has a calming, almost sedative quality. It binds to GABA receptors in the brain, producing a mild anti-anxiety effect. Synthetic progestins, the kind found in the pill and other hormonal methods, are not the same molecule. Different progestins bind to different receptors and behave quite differently. Some, like levonorgestrel, are more androgenic (testosterone-like), which can contribute to acne, oiliness, and in some women, irritability or low mood. Others, like drospirenone (found in brands like Yaz and Yasmin), are anti-androgenic but carry a slightly higher blood clot risk.
This variability explains why one woman can thrive on the pill she has been using for years while her sister feels like a completely different person on the same formulation. Hormonal response is deeply individual, shaped by genetics, gut health, liver enzyme activity, and baseline hormone levels. There is no universal "right" pill—which is why trial and error, while frustrating, is part of the process for so many women.
Important Note
Not all progestins are the same. If you are experiencing mood changes, low libido, skin changes, or persistent fatigue on your current birth control, the specific progestin formulation may be the issue — not hormonal contraception as a category. A conversation with your doctor about switching formulations is always worth having.
What Happens to Libido — And Why
Low libido is one of the most commonly reported—and most commonly dismissed—complaints among women on hormonal birth control. The explanation is both hormonal and structural. Estrogen and testosterone both drive desire. Combined pills suppress ovarian testosterone production, and because they raise a protein called sex hormone-binding globulin (SHBG), even the testosterone that remains gets "captured" and made unavailable to tissues. For some women, this drop in free testosterone is barely noticeable. For others, it can feel like the off switch was flipped.
What makes this more complicated is that elevated SHBG levels can persist for months—even years—after stopping the pill in some women. Research published in the Journal of Sexual Medicine found that SHBG levels in long-term pill users did not fully return to normal for some women even six months after discontinuation. This is an area where more research is genuinely needed, and where women deserve honest conversations with their doctors rather than reassurances that everything returns to normal immediately after stopping.
Hormonal Health Reference
How Common Birth Control Methods Affect Key Hormones
This table is for general educational reference only. Individual hormone responses vary. Speak with your healthcare provider for personalized guidance.
Mood, the Pill, and the Conversation We Keep Having
For decades, women who complained of depression or anxiety on the pill were often told it was all in their heads. That is no longer a defensible position. A large 2016 Danish study following over one million women found a statistically significant association between hormonal contraceptive use and subsequent depression diagnoses and antidepressant prescriptions. The association was strongest in adolescents and in women using progestin-only methods.
This does not mean the pill causes depression in every woman—or even in most. But it does mean that when a woman reports feeling unlike herself on hormonal birth control, that experience deserves to be taken seriously. The brain is a hormone-sensitive organ. Estrogen and progesterone receptors are found throughout the limbic system, the emotional processing center of the brain. It would be surprising if synthetic hormones had no effect on mood at all.
Some women feel genuinely better on the pill—particularly those who experienced severe PMS or the depressive episodes associated with premenstrual dysphoric disorder (PMDD). For them, eliminating the wild hormonal swings of an ovulatory cycle brings real relief. The experience is not universal, and that is precisely the point.
Did You Know?
The brain contains estrogen and progesterone receptors in the hippocampus—the region central to memory and emotional regulation. This is why many women report changes in memory recall, emotional processing, and social sensitivity as their hormones shift through their cycle—or when synthetic hormones are introduced.

Coming Off Birth Control: What to Expect
Post-pill recovery is its own hormonal story. Most women's cycles return within one to three months after stopping combined hormonal birth control, but the transition is rarely seamless. In the short term, it is common to experience a surge in sebum (leading to breakouts), heavier or more crampy periods, and a pronounced return of PMS symptoms that had been masked by the pill's leveling effect.
Some women experience a condition informally called "post-pill syndrome"—a cluster of symptoms including irregular cycles, hair thinning, and persistent acne that can last for several months. While not a formal clinical diagnosis, the experience is real. Nutritional support, particularly zinc, magnesium, and B vitamins depleted by long-term pill use, may help ease the transition. This is a conversation worth having with a functional medicine practitioner or an OB-GYN who takes a whole-body approach.
Women with underlying PCOS or thyroid conditions may find that coming off the pill unmasks symptoms that had been quietly suppressed. In some cases, a PCOS diagnosis only becomes clear after stopping hormonal birth control. This is not a failure of the medication—it is information your body has been waiting to share.
Knowing Your Options
The conversation about birth control has matured significantly. Women today have more options than any previous generation, and more access to information about what those options actually do inside the body. The copper IUD remains the most effective hormone-free option, preserving your natural cycle entirely while offering over 99% efficacy. Fertility awareness-based methods, when practiced correctly and consistently, are also gaining renewed attention—partly because of better app-based tracking tools and partly because more women simply want to understand their bodies rather than override them.
Barrier methods, used consistently, carry no hormonal burden at all. And for women who do choose hormonal contraception, there is genuine variation in how different formulations feel—enough that if one method is not working for you physically or emotionally, exploring another is a legitimate and reasonable step.
The NHS Contraception Guide offers one of the clearest publicly available breakdowns of the full range of contraceptive methods, including how each works and what to expect in terms of side effects and return to fertility—useful reading before any appointment.
What you deserve, in any of these choices, is honesty. Honesty about the trade-offs, the side effect profiles, the individual variation, and the fact that your experience of your own body is data worth taking seriously. No contraceptive method should make you feel like a stranger to yourself—and if it does, that is not a small thing to live with. It is a reason to go back to your doctor and keep asking questions until you find what actually works for you.
Your Questions Answered: Birth Control & Hormones
Disclaimer: This content is for informational and educational purposes only and does not constitute medical advice. It is not intended to be a substitute for professional diagnosis or treatment. Always consult with a qualified healthcare provider regarding any medical condition or treatment plan. Never disregard professional medical advice because of something you have read here.





