 English
English  Español
Español  Português
Português 
Think back to your high school health class. If your experience was anything like most women's, you probably sat through a slideshow about reproduction, got a quick anatomical diagram that made everything look clinical and vaguely alarming, and left with more questions than answers.
Maybe someone mentioned STIs. Maybe they mentioned pregnancy. Almost certainly nobody mentioned pleasure, arousal, or what healthy desire actually feels like for a woman.
Decades later, the gap in that early education shows up in quiet ways — in women who feel disconnected from their own bodies, who don't know what "normal" looks like for them, or who carry unnecessary shame around perfectly natural experiences. This isn't a lecture. It's a catch-up conversation — the one many of us never got.
"Almost certainly nobody mentioned pleasure, arousal, or what healthy desire actually feels like for a woman."
— Lexi PierceYour Anatomy, Beyond the Basics
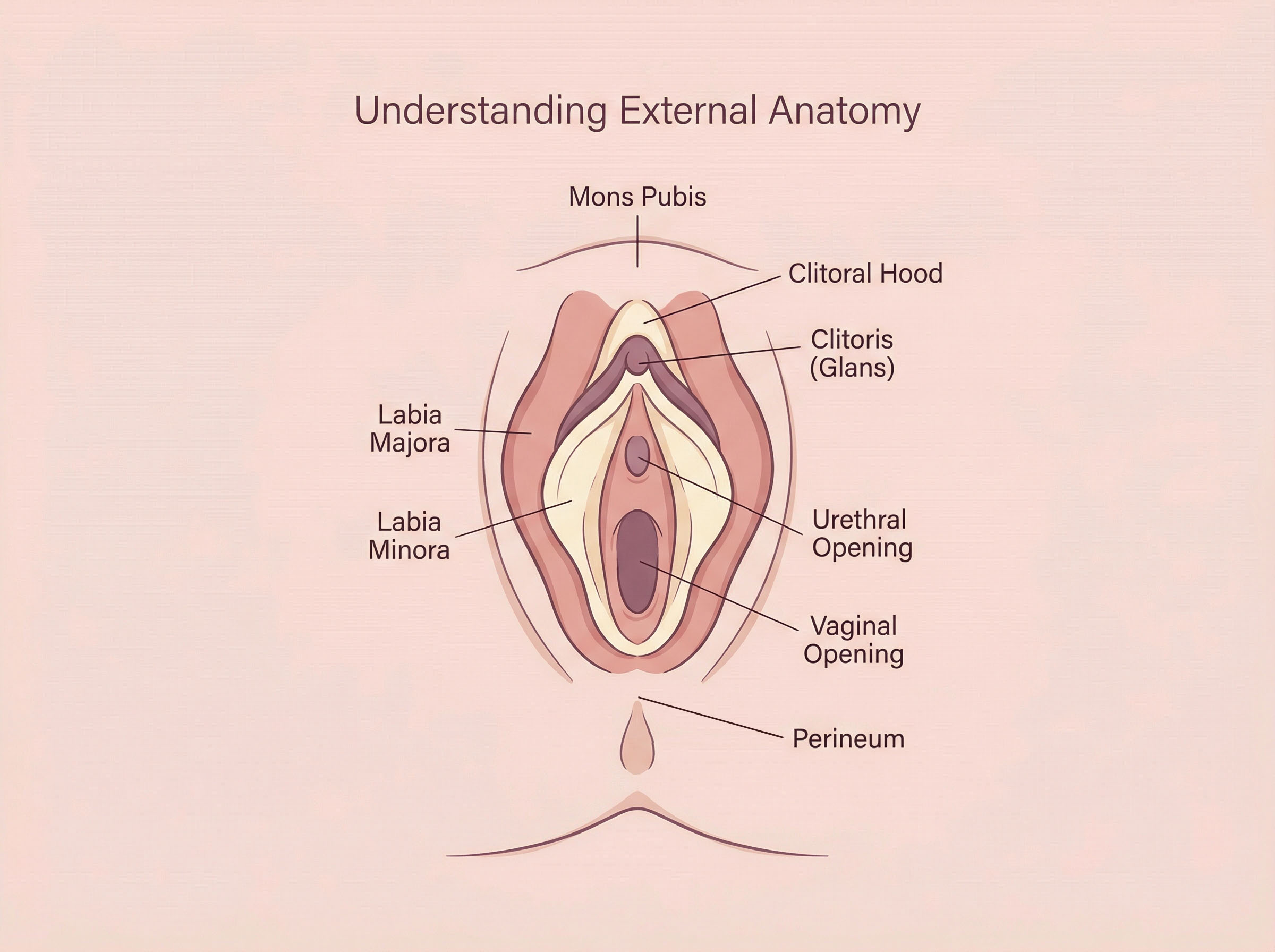
Most diagrams in school focused on the internal reproductive system — uterus, ovaries, fallopian tubes — with zero attention paid to the external anatomy that plays a significant role in a woman's sexual experience. Understanding your own body is not indulgent; it's practical.
The vulva refers to all of the external female genitalia. This includes the labia majora (outer lips), labia minora (inner lips), the clitoral hood, the clitoris, and the vaginal opening. Enormous variation exists in how these structures look — size, shape, color, and symmetry all differ from woman to woman, and that range is entirely normal to a certain extent.
The clitoris deserves its own paragraph. What most people were shown in school — a tiny external nub — is only the visible tip of a much larger internal structure. The clitoris has two internal "legs" (crura) and two "bulbs" that extend inward on either side of the vaginal canal. This internal structure is why indirect stimulation — pressure, friction nearby — can feel so effective. The clitoris contains approximately 8,000 nerve endings, making it exquisitely sensitive and central to sexual pleasure for the majority of women.
How Arousal Actually Works
Arousal is not simply a switch that flips from off to on. For women, it tends to be more of a gradual process — one that involves both the body and the mind together.
When a woman becomes aroused, blood flow increases to the genitals, causing the clitoris and labia to swell slightly (this is the female equivalent of an erection). The vaginal walls begin to produce natural lubrication — a process called vaginal transudation — which reduces friction and increases comfort. The vaginal canal also lengthens and expands in a process called "tenting," preparing for potential penetration.
But here's what many women don't realize: physical arousal does not always match subjective desire. You can feel physically lubricated without feeling emotionally ready, or feel genuine desire without obvious physical signs. Researchers call this a "concordance gap," and it's far more common in women than in men. This doesn't mean something is wrong — it means the body and mind operate on related but distinct tracks, and understanding both matters.
Studies show that only about 18% of women reliably reach orgasm through penetration alone. For most women, direct or indirect clitoral stimulation is the most reliable path to climax — a fact that sexual health researchers have documented for decades but that rarely makes it into mainstream conversation.
Desire: It Comes in Different Forms
Many women grow up with the impression that "normal" desire works the way it does in films — spontaneous, urgent, and instantly physical. In reality, sexual desire operates in more than one way, and understanding the difference can save a lot of unnecessary worry.
Spontaneous desire is the type that arises seemingly out of nowhere — a random thought, an image, or a moment that triggers arousal without obvious cause. This model tends to be more common in men and in younger women.
Responsive desire is arousal that emerges in response to stimulation — a touch, a kiss, an intimate moment that begins to unfold. Many women, particularly after having children or during periods of stress or hormonal change, find that their desire is primarily responsive. This is not a deficiency. It simply means that the conditions need to be right before desire kicks in, which is biologically and psychologically well within the range of normal.
Knowing which type of desire you tend to experience can actually improve your intimate life considerably. If you're a responsive-desire woman waiting for spontaneous arousal before initiating, you may wait a long time — and misread that waiting as a problem with your relationship or yourself.
Infographic
Two Pathways to Desire
Spontaneous Desire
Arises without obvious external trigger. More common in men and younger women. Often misread as the "only" normal type.
Responsive Desire
Emerges in response to intimacy and stimulation. Very common in women, especially after children or during life transitions. Completely normal.
Both are normal. Neither means something is missing.
Consent: More Than a Yes or No
Consent gets talked about a lot in the news, but often in very narrow terms — usually as a legal threshold rather than a living part of a healthy relationship. In practice, consent within an established relationship is ongoing, dynamic, and communicated in many ways beyond a single word.
Healthy consent includes the freedom to change your mind. Agreeing to something once doesn't obligate you for future occasions. Consent given under pressure, out of obligation, or from a place of fear is not genuine consent — and a healthy partner will not only hear a "no" but actively make space for one.
For women who grew up in environments where their boundaries weren't modelled or respected, recognizing and voicing their own limits can feel unfamiliar. The work of building that skill — knowing what you want and don't want, and feeling entitled to say so — is its own form of adult sexual education.
📌 Call Out
What Genuine Consent Looks and Sounds Like
- It is freely given — not extracted through pressure or persistence
- It can be withdrawn at any moment, for any reason, without explanation
- It applies to each individual act, not an entire encounter
- Silence or absence of refusal is not the same as agreement
- It exists within long-term relationships just as much as new ones
First Experiences: What to Know Before and After
Whether you're approaching a first sexual experience or reflecting on one that happened years ago, there are a few things worth knowing that might have reframed things had someone told you earlier.
The hymen is widely misunderstood. It is a thin, flexible membrane that partially covers the vaginal opening — and it does not "break" like a seal when a woman first has sex. It stretches. In many women, the hymen has already stretched or worn thin through physical activity, tampon use, or simply through normal development. Bleeding during first intercourse is not universal, not required as evidence of virginity, and not always due to the hymen — it can result from insufficient arousal and lubrication, causing small tears in vaginal tissue.
Pain during first intercourse is common but not inevitable. If there is adequate arousal, sufficient natural or added lubrication, and a patient, attentive partner, the first experience can be comfortable. Ongoing pain with penetration — whether a first experience or a recurring one — is worth discussing with a healthcare provider, as several treatable conditions can cause it.
Emotional complexity is normal. First sexual experiences carry a lot of social weight, and women often feel pressure to feel a certain way afterward — liberated, or bonded, or transformed. The truth is that emotional responses vary enormously, and whatever you feel is valid. Some women feel closer to their partner. Some feel fine but underwhelmed. Some feel a complicated mix. Give yourself the grace to respond authentically.
Sexual Health Basics: What to Know at Any Age
Pleasure as a Legitimate Part of Sexual Health
For a long time — and in many households still — the idea that women's pleasure matters on its own terms was either ignored or treated as secondary. Sexual health messaging focused almost entirely on risk avoidance: don't get pregnant, don't get an STI. The idea that sex should feel good for women, and that understanding how to make that happen is a worthwhile pursuit, rarely got equal airtime.
But pleasure is not a bonus feature of sexuality. It's part of why intimacy matters to people — it bonds partners, relieves stress, improves mood, and contributes to overall relationship satisfaction. Research has consistently linked sexual satisfaction with broader wellbeing, particularly for women in committed relationships.
Practically speaking, this means knowing your own body — what kinds of touch you find comfortable, what you enjoy, and what you don't — is not self-indulgent. It's information that makes you a more communicative partner and a more self-aware person. And communicating that information to a partner, even though it can feel vulnerable, tends to improve sexual experiences considerably for both people involved.

The Pelvic Floor: An Overlooked Player
If you've had children, you've probably heard about the pelvic floor — usually in the context of postpartum recovery or leakage when you sneeze. But the pelvic floor plays a significant role in sexual experience as well, and it rarely gets discussed in that context.
The pelvic floor is a group of muscles that form a hammock-like base at the bottom of the pelvis. These muscles support the bladder, uterus, and bowel. During sexual arousal, the pelvic floor muscles naturally increase in tension. During orgasm, they contract rhythmically. After, they relax.
In some women, these muscles are too tight — a condition called hypertonic pelvic floor — which can cause discomfort or pain during penetration, difficulty with tampon insertion, or persistent pelvic aching. In others, reduced tone following childbirth can affect sensation. Both situations are treatable through pelvic floor physiotherapy, a specialised form of care that is still underutilized largely because few women know it exists.
🌍 Cultural Insight
How Other Cultures Approach Women's Sexual Education
In the Netherlands, comprehensive sexual education begins around age 4 with age-appropriate lessons in body autonomy and continues through adolescence with frank discussion of anatomy, pleasure, and consent. The result? Dutch young people consistently report higher rates of positive first sexual experiences and better communication with partners.
In contrast, many English-speaking countries have historically taken an abstinence-emphasis approach, which research repeatedly shows is less effective at either delaying sexual activity or promoting healthier outcomes when it does occur.
Sexual Health Across Life Stages
Sexual health is not static. It shifts across hormonal cycles, through pregnancy and postpartum periods, during perimenopause and menopause, and with age. Understanding that these shifts are normal — rather than signs of permanent loss — changes how women experience and respond to them.
Across the monthly cycle, oestrogen and testosterone fluctuate in ways that affect desire. Many women notice increased libido around ovulation, a dip before menstruation, and variation in how touch feels at different points. Tracking these patterns isn't obsessive — it's useful information.
Postpartum, many women experience reduced desire as prolactin (the hormone that supports breastfeeding) suppresses oestrogen and testosterone. Vaginal dryness is common during this period. These are physiological responses, not indicators of relationship trouble, and most resolve naturally as hormones rebalance.
During perimenopause and menopause, declining oestrogen levels can lead to vaginal atrophy — thinning and drying of vaginal tissue — which makes intercourse uncomfortable. This is one of the most under-treated conditions in women's health, largely because women don't know to ask for help. Effective treatments exist, and a conversation with a knowledgeable GP or gynaecologist can make an enormous difference.
🚀 Quick-Start Guide
Your Adult Sexual Education: Where to Begin
✅ Do
- Learn your own anatomy — a mirror is a simple starting point
- Track your cycle and notice how desire shifts
- Use a water-based lubricant if intercourse is uncomfortable
- Communicate openly with your partner about what you enjoy
- See a pelvic floor physiotherapist if you experience pain with sex
- Speak to your GP about menopausal vaginal symptoms
❌ Don't
- Assume pain during sex is something to simply endure
- Compare your desire or response to anyone else's
- Mistake low spontaneous desire for a broken relationship
- Assume lubricant use means something is wrong with you
- Wait years before raising sexual health concerns with a doctor
- Fake responses — it hinders communication and your own experience
Talking to Your Partner: It Doesn't Have to Be Awkward
Many women find it easier to navigate difficult conversations at work than to tell a partner what they enjoy in bed. This isn't a character flaw — it's a product of the messages most of us absorbed growing up, where women's desires were either absent from the script or framed as something to be managed rather than expressed.
The good news is that communication around intimacy gets easier with practice, and the stakes tend to feel lower once you've done it a few times. A few principles that help: start outside the bedroom when possible, use "I notice" or "I love it when" framing rather than criticism, and be specific. "I'd love it if we slowed down a little" is more useful than a vague sense of dissatisfaction that never gets voiced.
It's also worth knowing that most partners — when they genuinely care — want this feedback. No one who loves you wants to be doing something you don't enjoy. The conversation, however briefly uncomfortable, tends to open doors rather than close them.
"No one who loves you wants to be doing something you don't enjoy. The conversation, however briefly uncomfortable, tends to open doors rather than close them."
— Lexi PierceWhen to Seek Professional Support
There are certain experiences that go beyond what self-education can address, and that deserve professional support. These include persistent pain with penetration or intercourse, a notable and unexplained change in desire, discomfort that worsens over time, difficulty reaching orgasm that causes distress, or sexual anxiety that significantly affects your relationship.
A GP, gynaecologist, or sexual health specialist is the right starting point. For emotional or relational elements, a therapist who specialises in sexual health or couples therapy can be enormously helpful. These are medical and psychological issues like any other — and treating them as such, rather than something to silently manage, tends to produce much better outcomes.
The International Society for the Study of Women's Sexual Health (ISSWSH) maintains a directory of specialist providers and publishes patient-facing information that is evidence-based and written in plain language. It's a strong starting point for anyone looking for qualified guidance.
📊 By the Numbers
What Research Actually Shows
of women reliably reach orgasm through penetration alone
nerve endings in the clitoris — more than any other human body part
of women report experiencing low desire at some point — most cases are situational
women experience clinically significant sexual pain — yet most never raise it with a doctor
The Education That Was Always Yours to Have
None of this information is secret. It exists in medical literature, in the offices of knowledgeable healthcare providers, and in books written by people who spent careers studying women's sexual health. What has been missing, for too many women, is the permission to seek it out — the sense that this knowledge is relevant to them and that their questions deserve answers.
They always have. Whether you're 22 or 52, newly partnered or long married, curious or actively struggling with something — the information in this article is not too late to be useful. Consider it the class that was always overdue.
📋 In Brief
Key Takeaways from This Article
- The clitoris is far larger than most school diagrams show, and it's central to pleasure for most women
- Responsive desire — arousal that emerges from context rather than appearing spontaneously — is common and completely normal in women
- Physical arousal and subjective desire don't always align, and that's not a malfunction
- Pain during sex is common but not inevitable, and treatable causes exist
- Consent is ongoing, applies within all relationships, and can always be withdrawn
- The pelvic floor muscles affect both sexual sensation and comfort — pelvic physiotherapy is an underused resource
- Hormonal shifts across the monthly cycle, postpartum period, and menopause all affect sexual experience in predictable, manageable ways
- Communicating with a partner about your preferences is one of the most effective things you can do for your intimate relationship
Frequently Asked Questions
Disclaimer: This content is for informational and educational purposes only and does not constitute medical advice. It is not intended to be a substitute for professional diagnosis or treatment. Always consult with a qualified healthcare provider regarding any medical condition or treatment plan. Never disregard professional medical advice because of something you have read here.





