 日本語
日本語  Deutsch
Deutsch  English
English  Español
Español  Français
Français  Português
Português 
Search the internet long enough and you will find claims that stretch credibility — measurements that sound more like urban legend than laboratory finding. The question of how large a clitoris can actually become is one that surfaces repeatedly in health forums, anatomy discussions, and curious midnight searches.
And yet the answer, when traced back to peer-reviewed medicine, is far more grounded, far more human, and far more interesting than the sensational headlines suggest.
This article follows the evidence. No shock value, no anatomy-class embarrassment, just clear science and honest conversation about a part of the body that remains one of the most under-researched in medicine — despite belonging to roughly half the world's population.
"The clitoris is one of the most under-researched organs in medicine — despite belonging to roughly half the world's population."
— Lexi Pierce, Women's Health
What Is Considered 'Normal' Clitoral Size?
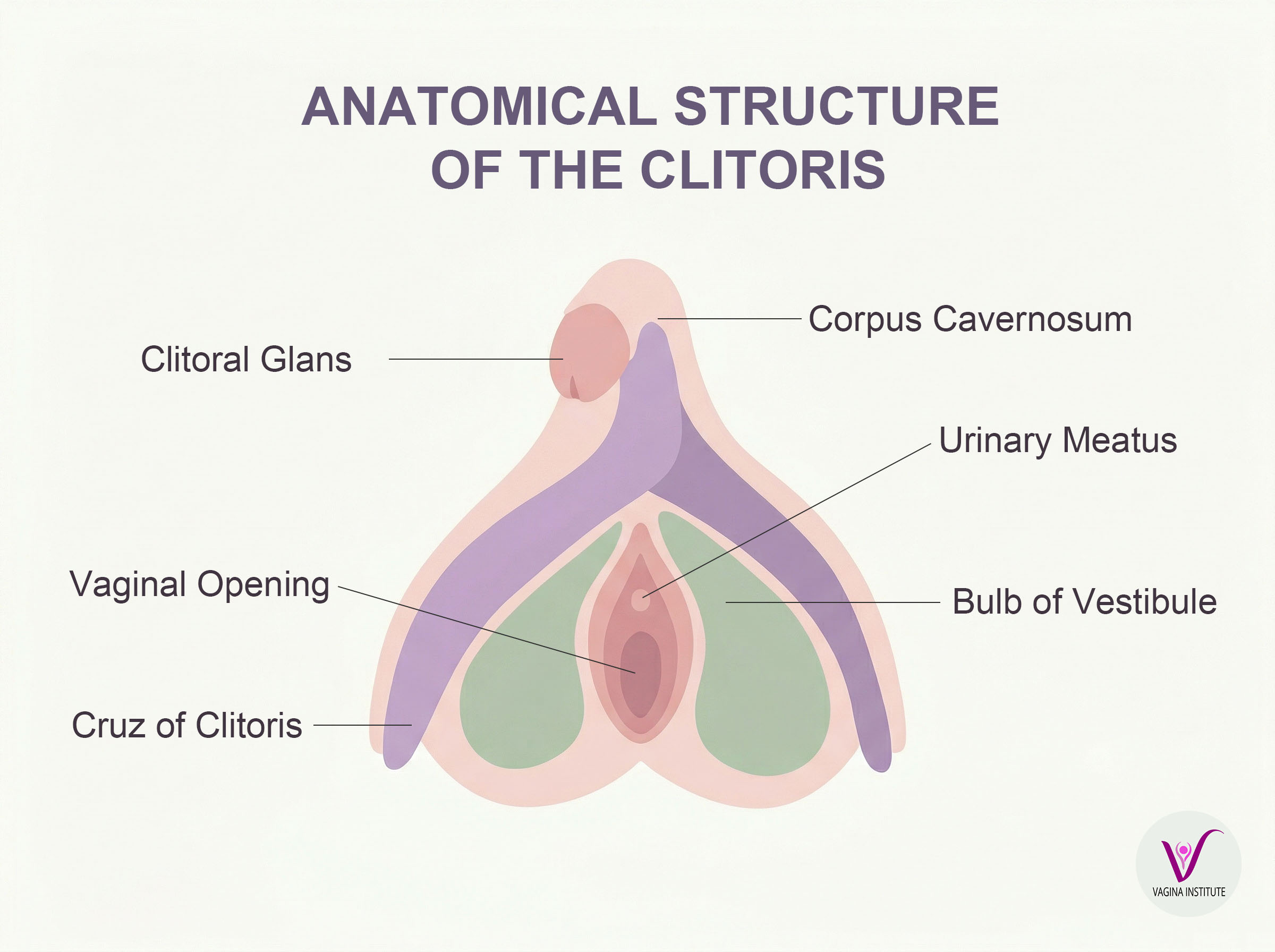
Before discussing extremes, it helps to understand what medicine actually considers typical. The clitoris is far larger than most anatomy diagrams have historically shown. What is visible externally — the glans, or tip — is only a small portion of a structure that extends internally, wrapping around the vaginal canal with two crura (legs) and two vestibular bulbs.
Research published in the Journal of Urology and subsequent ultrasound studies have found that the visible glans clitoris in adult women averages roughly 1.5 to 2 centimetres in length when not aroused, and approximately 0.5 to 1 centimetre in width. However, studies consistently show enormous natural variation — measurements ranging from under 1 centimetre to more than 3.5 centimetres fall within ranges documented in healthy women with no underlying condition.
Clitoral size is also known to change with age and hormonal shifts. Women who have given birth, women going through perimenopause, and women in their post-reproductive years all show measurable differences compared to younger, nulliparous women. In other words, the body changes — and that is entirely expected.
Reference Guide
Sources: Journal of Urology; BJU International; American Journal of Obstetrics & Gynecology. For general reference only — not a diagnostic tool.
The Largest Documented Cases
Medical literature does contain documented cases of significant clitoral enlargement, and they deserve to be discussed with the same clinical seriousness given to any other anatomical variation.
Case reports in peer-reviewed gynaecology and endocrinology journals describe clitoral measurements ranging from 4 centimetres to over 6 centimetres in length in women with conditions such as congenital adrenal hyperplasia (CAH) — a genetic condition present from birth that causes the adrenal glands to produce excess androgens (male sex hormones). In some of the more pronounced cases associated with severe untreated CAH or prolonged anabolic steroid use, measurements approaching or exceeding 5 to 6 centimetres of the glans have been recorded.
It is worth stating clearly: there is no single verified "world record" for clitoral size in any credible medical database. Claims circulating online — some citing measurements of 10 centimetres or more — do not correspond to published case studies.
The largest reliably documented cases in the peer-reviewed literature typically reach a maximum of 5 to 7 centimetres involving the corpora and glans, usually under specific medical conditions involving androgen excess. That said, this does not preclude the existence of clitorises exceeding 10 cm — for example, in theory through the combination of pre-existing congenital clitoromegaly and prolonged high-dose anabolic steroid use — or clitorises that can rival or even exceed the size of some smaller penises and potentially approach median erect penis length (approximately 13–14 cm). Given that there are over 4 billion women on Earth, the vast majority of clitorises have never been professionally measured, and the human body exhibits considerable natural anatomical variation that often remains undocumented.
What these cases share is a clinical context. They are not random outliers of human anatomy — they are the result of identifiable hormonal or genetic processes. That distinction matters.
✦ Did You Know?
The full clitoris — including its internal crura and vestibular bulbs — can measure up to 10 centimetres in total length in some women, even within the typical range. Most anatomy textbooks only depicted the visible glans until well into the 1990s. A complete anatomical description wasn't published until researcher Helen O'Connell's groundbreaking MRI work in 1998.
What Causes Clitoromegaly?
Clitoromegaly is the medical term for a clitoris that is enlarged beyond the established clinical threshold — generally accepted as a glans length greater than 3.5 centimetres in an adult woman. It is not a disease in itself, but a physical finding that usually indicates something worth investigating.
Congenital Adrenal Hyperplasia (CAH) is the most common cause in female newborns and children. This inherited condition disrupts the adrenal glands' ability to produce cortisol, leading to a compensatory overproduction of androgens. In female infants, excess androgens during foetal development can cause the clitoris to enlarge significantly, sometimes resembling male genitalia — a condition referred to as atypical or ambiguous genitalia. CAH is detectable through newborn screening programmes in many countries.
Polycystic ovary syndrome (PCOS), one of the most common hormonal conditions affecting women of reproductive age, can in some cases be associated with mild clitoral enlargement due to excess androgen production, though this is not a defining feature of the condition.
Anabolic steroids and testosterone therapy are well-documented acquired causes. Women who use anabolic steroids — whether for athletic performance or bodybuilding — or who receive testosterone as part of hormone therapy may experience measurable clitoral growth. This is a known and documented side effect, and the degree of enlargement generally correlates with dosage and duration of use.
Androgen-secreting tumours of the ovaries or adrenal glands can produce elevated androgen levels and cause rapid-onset clitoromegaly, which is one reason clinicians take a new or sudden enlargement seriously — particularly when accompanied by other signs of androgen excess such as voice deepening or increased body hair.
Less commonly, certain medications, neurofibromatosis (a genetic nerve-tissue condition), and trauma-related tissue changes have been cited in case literature as contributing factors.
🌿 Cultural Insight
Ancient Anatomy, Modern Silence
For centuries, female anatomy was described through a male lens — literally. Early anatomists named structures after their male counterparts and largely ignored the clitoris in published texts. Even the word clitoris appears in Western medical literature only from the 16th century, derived from the Greek kleitoris.
In many traditional cultures, the clitoris was acknowledged — and even celebrated — in fertility rituals. Its deliberate erasure from Western medical education is a relatively modern phenomenon, one that researchers like Helen O'Connell have spent careers correcting through anatomical MRI studies.
Can Size Change Over Time?
Yes — and this surprises many women when they first learn it. Clitoral size is not fixed across a lifetime. Hormonal changes at various life stages produce measurable differences.
During puberty, rising oestrogen and androgen levels cause the clitoris to grow alongside other secondary sexual characteristics. Studies using ultrasound have shown that the clitoris continues to increase in size through young adulthood, with some research suggesting peak size occurs in the mid-to-late twenties.
Pregnancy and childbirth also affect clitoral anatomy. Increased blood flow to the pelvic region during pregnancy can cause temporary engorgement, and some women report a lasting change in sensation or appearance after delivery, though long-term data on structural changes is limited.
Menopause brings a well-documented decrease in oestrogen, which leads to atrophy of genital tissues — the clitoris included. The glans may reduce in size and the hood (prepuce) can become less distinct. This is part of the broader condition known as genitourinary syndrome of menopause (GSM), which also affects vaginal tissues and lubrication.
In short: the clitoris ages alongside the rest of the body, responding to the same hormonal rhythms that shape female physiology throughout life.
Myths vs. Reality About Size
Perhaps no area of female anatomy has been more distorted by popular culture — and particularly by adult entertainment — than the clitoris. A few persistent myths are worth addressing plainly.
Myth: What you see in adult content represents normal anatomy. It does not. The bodies depicted in adult films are selected for specific visual characteristics and are not representative of the range seen in clinical practice or everyday life. Production editing further distorts reality. Many women have compared their anatomy to these images and concluded something is wrong with them — when in fact they fall entirely within typical variation.
Myth: A larger clitoris is always the result of sexual activity or arousal patterns. Not supported by science. Size during non-aroused states is determined by anatomy and hormones, not frequency of stimulation. Arousal does cause temporary engorgement — blood flow increases and the structure becomes more prominent — but this is temporary and leaves no permanent structural change.
Myth: Clitoromegaly is always visible and obvious. Not necessarily. The clitoral hood (prepuce) covers the glans in most women, and the degree to which the glans is exposed varies considerably. A clinician measuring for clitoromegaly does so under specific, standardised conditions — not by casual observation.
Myth: A larger clitoris means higher sex drive. There is no established correlation between glans size and libido in the medical literature. Sexual desire is governed by neurological, hormonal, psychological, and relational factors — not anatomical measurement.
📋 In Brief — What the Science Actually Shows
- Normal clitoral glans size ranges widely — roughly 1 to 3.5 cm in most adult women
- Clitoromegaly (clinical enlargement) begins above approximately 3.5 cm and has identifiable medical causes
- The largest reliably documented cases in peer-reviewed literature involve women with CAH or steroid exposure
- Online claims of extreme sizes often lack a verifiable medical source
- Clitoral anatomy changes throughout life in response to hormones — this is normal
- Size has no established connection to sexual sensitivity or libido
When Should Someone See a Doctor?
Most women will never need to give their clitoral anatomy a second thought from a medical perspective. Natural variation is just that — natural. But there are specific situations where a consultation with a gynaecologist or endocrinologist is genuinely worth pursuing.
A sudden or rapid change in clitoral size in an adult woman warrants attention, particularly if it is accompanied by other signs of androgen excess — increased facial or body hair, acne, voice changes, or irregular periods. These signs together can indicate an androgen-secreting tumour or another endocrine condition that benefits from early diagnosis.
In newborns and infants, atypical genital development — including a noticeably enlarged clitoris — is evaluated by paediatricians and paediatric endocrinologists as part of standard newborn assessment. CAH in particular requires prompt diagnosis because it can also affect salt regulation in the body with serious consequences if untreated.
Women who are using or considering testosterone therapy or anabolic steroids should discuss clitoral changes — along with all androgenic effects — with a physician before and during use. These changes, while often partial, are not always fully reversible.
For women who experience discomfort, pain, or distress related to clitoral size or sensitivity for any reason, gynaecological evaluation is always appropriate. The conversation about female anatomy is one that medical professionals are trained to have with compassion and clinical precision.

Frequently Asked Questions
The science of clitoral anatomy is still catching up to decades of medical neglect. What researchers now know — thanks largely to imaging technology that simply did not exist in earlier eras — is that the structure is more complex, more variable, and more fascinating than most of us were ever taught. Understanding that variation exists, that it has identifiable causes when it reaches clinical extremes, and that it rarely requires intervention, is the kind of knowledge that belongs in every woman's general health toolkit.
If you have questions about your own anatomy, a conversation with a gynaecologist is always the right place to start. Anatomy is not something to be embarrassed about. It is simply the body doing what bodies do — quietly, precisely, and in its own individual way.
Disclaimer: This content is for informational and educational purposes only and does not constitute medical advice. It is not intended to be a substitute for professional diagnosis or treatment. Always consult with a qualified healthcare provider regarding any medical condition or treatment plan. Never disregard professional medical advice because of something you have read here.
